Retinopathy of prematurity (ROP)
What is retinopathy of prematurity?
Retinopathy of prematurity is an eye disease that affects some babies who are born very early (premature) or have a birth weight under three pounds. ROP is the medical abbreviation for retinopathy of prematurity.
When a baby has ROP, the blood vessels in their retinas aren't growing the way they should.
The retina is a layer of special cells along the back wall of the eye. These cells send light signals to the brain so you can see. When there's a problem with the retina's blood vessels, it's called retinopathy.
Most babies with ROP get better on their own without treatment, but severe ROP needs to be treated by an eye doctor. Early treatment could help protect a newborn's eyesight for the rest of their life.
Causes and risk factors
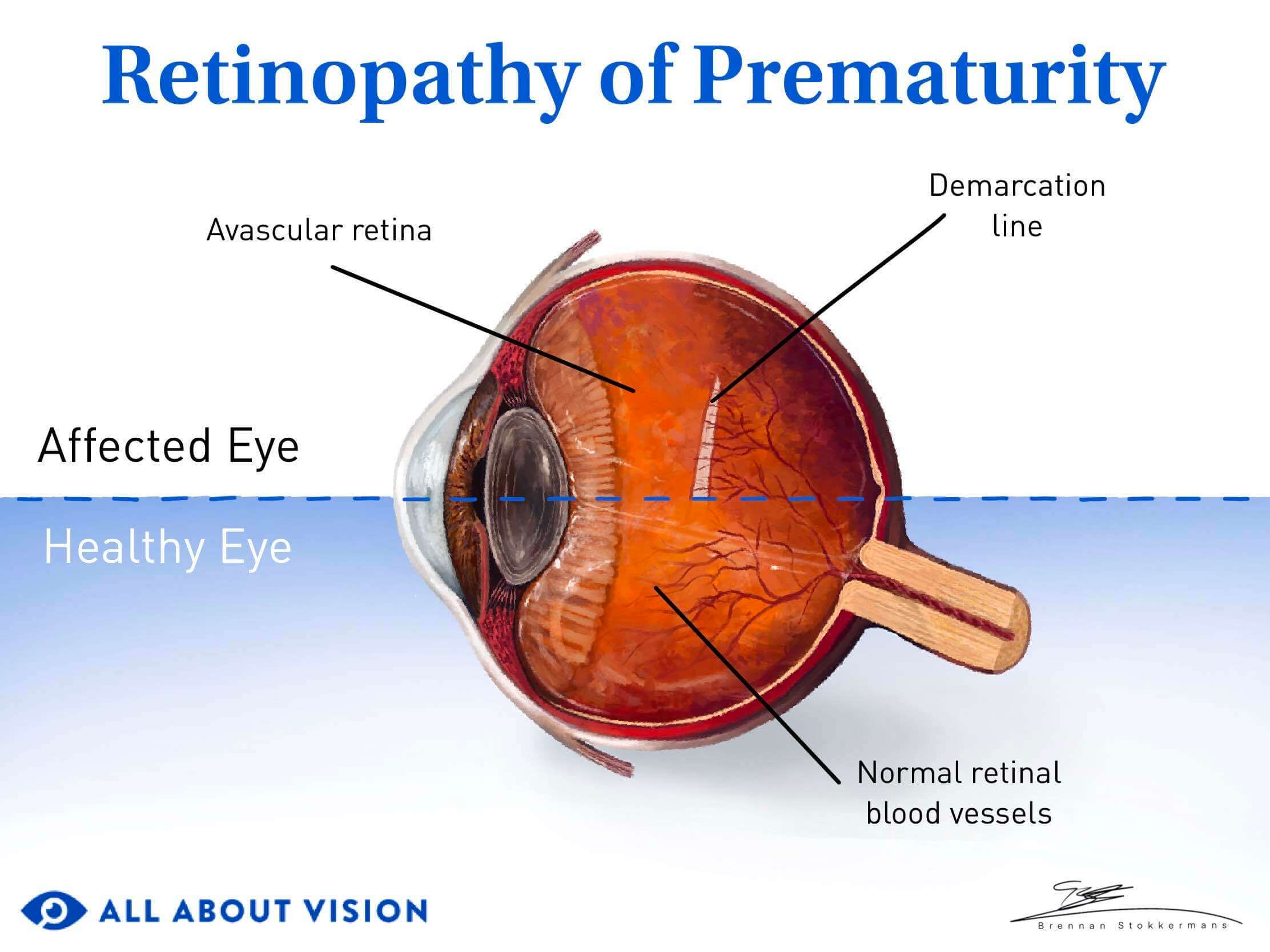
Retinopathy of prematurity is caused by unusual blood vessel growth in a newborn's retinas. When ROP is severe, the new blood vessels can pull the retina away from the eye wall and damage a newborn's eyesight.
The main risks for retinopathy of prematurity are:
Very early delivery – During or before the 30th week of pregnancy
Low birth weight – Less than three pounds
A baby's retinas start developing many months before they're born, and they keep growing until shortly before they reach full term (week 39-40).
A preemie's eyes may not have a chance to develop all the way, especially if they're born many weeks before full term. Early exposure to light, different temperatures and other factors can also change the way their eyes develop.
Other health problems that could contribute to ROP include:
Breathing problems (may be related to conditions like respiratory distress syndrome and the extra oxygen used to treat them)
Other health conditions that affect a newborn's brain, heart or other vital parts of the body
Infections
Low iron levels (anemia)
Low vitamin E levels
Is ROP common?
Mild retinopathy of prematurity is common in preemies who have very low birth weight.
One study of premature babies in the United States showed:
Two-thirds of newborns who weigh less than 2.75 pounds have some level of ROP.
One in 10 of these newborns have severe ROP that needs treatment.
About 3%-4% of babies with ROP become legally blind.
The more underweight a baby is at birth, the more at risk they are of having ROP.
Signs and symptoms
You probably won't be able to see any retinopathy of prematurity symptoms on the outside. An eye doctor needs to look into your newborn's eyes to check for signs of ROP.
If a baby had severe ROP as a newborn, you might notice certain signs later on:
They don't follow objects with their eyes.
They don't respond to light normally.
Their eyes look crossed or misaligned (strabismus)
Their eyes look like they're shaking or moving back and forth (nystagmus).
Their pupils look white instead of black.
Testing and diagnosis
ROP should be diagnosed early on so the doctor can start treatment (if needed) as soon as possible.
Diagnosing retinopathy of prematurity
The American Association for Pediatric Ophthalmology and Strabismus recommends an ROP eye exam (also called an ROP screening) if a newborn meets these conditions:
They're born before the 31st week of pregnancy.
They weigh less than 1,500 grams (about 3.3 pounds) at birth.
They have other health problems that put them at a higher risk for ROP.
Some preemies are screened for ROP in the hospital shortly after they're born. But the signs of ROP aren't always visible right away, so the eye doctor may ask you to wait a few weeks.
Many doctors recommend scheduling an ROP exam when a premature infant is about four weeks old. This may be a little longer for some babies.
What happens during an ROP eye exam?
During a standard ROP exam, a pediatric ophthalmologist uses medicated eye drops to make a baby's pupils open wider.
This is called eye dilation. The effect goes away on its own within a few hours to a day.
Once their pupils are dilated, the doctor will look into their eyes to examine both retinas. If the doctor makes an ROP diagnosis, they will grade it from stage 1 to 5 based on how severe it is. This helps them decide if treatment is needed.
Follow-up exams
Your baby's eye doctor may need to repeat the exam every 1 to 3 weeks until their retinal blood vessels stop growing.
Some people who had ROP as babies have a higher risk of developing other eye conditions later in life. For this reason, their eye doctor will recommend scheduling one or more follow-up eye exams every year for the rest of their lives.
It's important to stick to this schedule so a doctor can address any new issues as soon as possible.
Retinopathy of prematurity stages
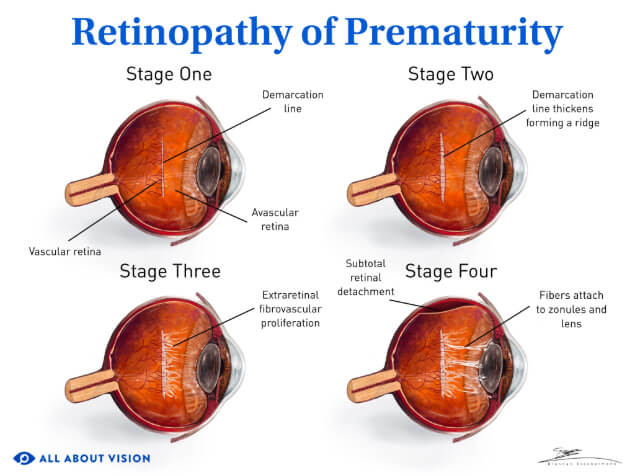
Eye doctors use five ROP stages to grade a baby's condition. The higher the stage number, the more the retina is affected.
The five stages of ROP are:
Stage 1 ROP
Stage 1 is the mildest level of ROP. Most babies with stage 1 ROP get better on their own and go on to have healthy eyesight.
Click image to enlarge.
Stage 2 ROP
Stage 2 is more advanced, but most babies recover without treatment and have healthy vision afterward.
Stage 3 ROP
In stage 3, extra blood vessels have started to grow on the retina. An eye doctor will treat the problem so it doesn't get worse.
Stage 4 ROP
In stage 4, part of the retina has pulled away from the back of the eye (retinal detachment). This needs to be treated right away.
Stage 5 ROP
Stage 5 is the most severe level of ROP because the retina has detached completely. This also needs emergency treatment.
Other ROP terms
Zones
Click image to enlarge.
Click image to enlarge.
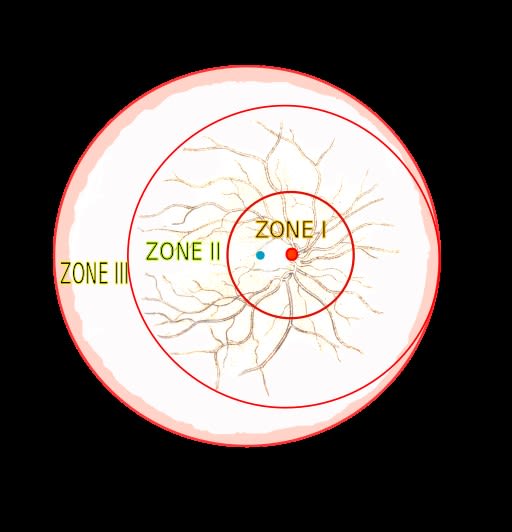
The zone is the area where ROP happens inside the eye.
Zone I is around the spot where the optic nerve connects to the retina (the optic disc). Zone II and zone III are outside of zone I.
Plus disease
Plus disease means the new blood vessels look enlarged and wavy. It's a sign of severe retina damage.
An eye doctor can diagnose plus disease with any stage of ROP.
Aggressive retinopathy of prematurity (A-ROP)
Aggressive ROP, also called A-ROP, is a fast-moving form of retinopathy of prematurity. This leads to severe blood vessel problems in a shorter amount of time.
Complications
Retinal detachment is the most concerning complication in babies with severe retinopathy of prematurity. It's a sight-threatening problem that needs to be treated very quickly.
Severe ROP usually makes the retina detach between 2 and 12 months after a baby is born. This is most common in newborns who weigh less than two pounds at birth.
Some babies will have a higher risk of retinal detachment later in their lives, too.
When the retina separates from the back of the eye, treatment can help protect as much eyesight as possible. Unfortunately, some babies go on to have significant vision loss or blindness, even with prompt treatment.
ROP can also cause macular folds. This condition affects the part of the retina (macula) that's responsible for the central area of your vision.
Some macular folds cause worsening eyesight, double vision or wavy vision. The eye surgeon may need to perform surgery to flatten the folds in the retina.
Other complications of ROP can happen later on. Some of them are:
Myopia – Objects look blurry when they're farther away (also known as nearsightedness).
Strabismus – Both eyes point in different directions (some forms are called "crossed eyes").
Amblyopia – One or both eyes have poor vision that doesn't get better with glasses (sometimes called "lazy eye").
Anisometropia – Each eye has a different vision prescription.
Management and treatment
Eye doctors often use one or two types of retinopathy of prematurity treatment for babies with severe ROP:
A laser procedure that carefully burns the retina to stop unusual blood vessel growth
Injections of anti-VEGF medicine into the eye that stop blood vessels from growing
Babies with severe ROP have to be treated quickly to prevent more damage. Doctors usually recommend treatment within three days of diagnosis.
A newborn with stage 4 or 5 ROP may need eye surgery to treat their detached retina. The surgeon may suggest one of these procedures:
Vitrectomy – The surgeon removes the gel-like fluid inside the eye and replaces it with salt water or a bubble. They also remove any scar tissue to help the retina heal.
Scleral buckle surgery – The surgeon attaches a flexible "belt" to the white part of the eye that gently squeezes it. This helps push the retina back into place so it can heal.
ROP surgery is usually performed by an eye surgeon who specializes in treating babies.
Can you prevent ROP?
Since premature birth is the main cause of ROP, some people can lower their baby's risk by avoiding an early delivery. But this isn't always possible, and some babies must be delivered early no matter what.
If possible, your doctor will give you more information about preventing a premature birth.
Questions to ask your baby's ophthalmologist
Try to prepare any questions for the ophthalmologist before the ROP screening. This can help you get the most out of your time with the doctor.
Consider asking:
Will my baby need any more screenings for ROP? If so, how many more exams may they need?
Will their ROP cause any vision symptoms? If so, how might it affect their eyesight now and in the future?
Are they at risk for a detached retina?
Do they need treatment? If so, are there any reasonable alternatives?
Once their ROP is treated or goes away on its own, should I watch for other eye problems as they grow up?
How often should I schedule an eye exam during their childhood and adolescence?
It can feel worrying to find out your baby has an eye condition like ROP. While most newborns improve on their own with healthy eyesight, some babies have a severe form of ROP that could harm their vision.
Your baby's eye doctor and health providers have training and experience specifically for this eye disease. They're here to help you navigate the process and achieve the best possible outcome for your baby.
Retinopathy of prematurity. National Eye Institute. November 2023.
Retina. A.D.A.M. Medical Encyclopedia [Internet]. April 2023.
Retinopathy. Harvard Health. September 2023.
Retinopathy of prematurity. Cleveland Clinic. August 2023.
Know your terms: Full-term pregnancy. National Child & Maternal Health Education Program. June 2022.
What is retinopathy of prematurity (ROP)? EyeSmart. American Academy of Ophthalmology. May 2023.
Respiratory distress syndrome (RDS). National Heart, Lung, and Blood Institute. March 2022.
Retinopathy of prematurity (ROP). Merck Manual Consumer Version. March 2024.
A review on the incidence and related risk factors of retinopathy of prematurity across various countries. Cureus. November 2022.
Retinopathy of prematurity. American Association for Pediatric Ophthalmology and Strabismus. April 2023.
Quick facts: Retinopathy of prematurity (ROP). Merck Manual Consumer Version. September 2023.
Retinopathy of prematurity. StatPearls [Internet]. September 2023.
Classifying retinopathy of prematurity. Review of Ophthalmology. July 2022.
Retinopathy of prematurity. EyeWiki. American Academy of Ophthalmology. January 2024.
Retinal folds: To operate or not to operate. Indian Journal of Ophthalmology. June 2020.
Macula lutea. A.D.A.M. Medical Encyclopedia [Internet]. November 2023.
Nearsightedness (myopia). National Eye Institute. November 2023.
Strabismus. A.D.A.M. Medical Encyclopedia [Internet]. August 2022.
Amblyopia. American Association for Pediatric Ophthalmology and Strabismus. January 2024.
Anisometropia. American Association for Pediatric Ophthalmology and Strabismus. April 2023.
Retinopathy of prematurity. MSD Manual Professional Version. March 2024.
What is vitrectomy? EyeSmart. American Academy of Ophthalmology. July 2023.
Scleral buckle. Cleveland Clinic. June 2023.
Page published on Thursday, October 24, 2019
Page updated on Tuesday, August 20, 2024
Medically reviewed on Tuesday, June 25, 2024